Guide
Comprehensive Guide to Intake Attribution and Call Quality
A practical framework for treatment center operators to track inquiry sources, score intake calls, and connect marketing spend to admissions outcomes.

Understanding Intake Attribution

Why knowing where your admissions actually come from changes everything
Intake attribution is the discipline of tracking every patient inquiry from its first marketing touchpoint through to admission. For behavioral health treatment centers, this is not an academic exercise. It is the difference between knowing which channels produce qualified admissions and guessing based on last-click data that tells you almost nothing useful.
Most treatment centers operate with a significant blind spot. They know how many calls came in. They might know which campaigns generated clicks. But the connection between a specific marketing dollar and a specific admission is often lost in the handoff between marketing platforms, call tracking systems, CRM records, and intake team notes. This gap costs money. According to the Substance Abuse and Mental Health Services Administration (SAMHSA), behavioral health facilities face increasing pressure to demonstrate outcomes and cost-effectiveness. Attribution is where that demonstration starts.
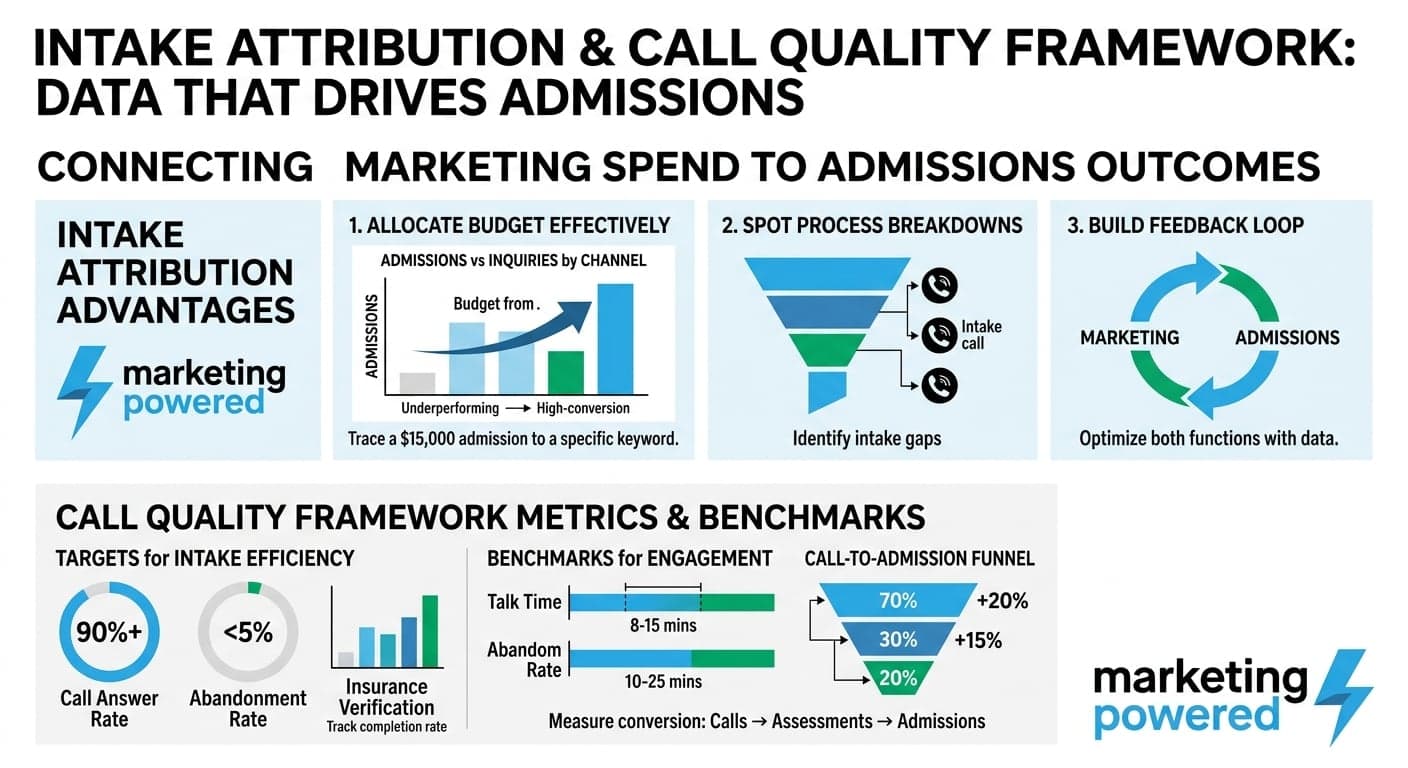
Correct intake attribution changes how you allocate budget. When you can trace a $15,000 monthly admission back to a specific keyword, ad group, or referral partner, you stop funding channels that produce inquiries but not admissions. You start doubling down on what actually works. Over $50M+ in managed lifetime spend across behavioral health marketing campaigns, the pattern is consistent: centers with disciplined attribution outperform those relying on platform-reported conversions by a wide margin.
The challenge is that behavioral health intake is not a single-touch conversion. A family member might search for treatment options, visit your site, leave, return three days later through a different device, call your intake line, and then take another week to make a decision. Traditional last-click attribution credits the final touchpoint and ignores every interaction that built trust along the way. Multi-touch attribution models distribute credit across the journey, but they require infrastructure that most centers do not have in place.
Treatment centers that implement proper intake attribution gain three immediate advantages. First, they identify which marketing channels produce admissions, not just calls. Second, they spot intake process breakdowns where qualified inquiries fail to convert. Third, they build a feedback loop between marketing and admissions that improves both functions over time. This is not about dashboards or reporting. It is about making decisions with data instead of assumptions.
Implementing a Call Quality Framework
Free Audit
Want a straight read on where your budget is leaking?
Building the infrastructure to measure what matters on every intake call
A call quality framework is a structured system for evaluating intake calls against defined standards. It includes scoring criteria, monitoring practices, feedback mechanisms, and continuous improvement processes. For treatment centers handling sensitive behavioral health inquiries, this framework must balance conversion optimization with compliance requirements and genuine care for callers in crisis.
The first step is defining what a successful intake call looks like at your center. This is not a generic checklist. It reflects your admissions criteria, your clinical model, your insurance verification process, and your center's specific value proposition. A successful call at a luxury residential program looks different from a successful call at a Medicaid-focused IOP. Your framework must match your operation.
Start by establishing clear benchmarks. These typically include call answer rate, abandonment rate, talk time distribution, conversion rate, and insurance verification completion rate. According to research from the National Institute on Drug Abuse (NIDA), the window for engaging someone seeking treatment is narrow. Your benchmarks should reflect that urgency.
- Call answer rate: Target 90%+ of calls answered within 20 seconds during business hours
- Abandonment rate: Keep below 5% with proper staffing and overflow protocols
- Talk time benchmarks: Initial intake calls typically range 8-15 minutes for qualified inquiries
- Conversion tracking: Measure calls to scheduled assessments, assessments to admissions
- Insurance verification: Track verification completion rate and time-to-verification
Call Quality Framework Implementation
Monitoring, feedback, and continuous improvement
Monitoring practices form the operational core of your framework. This means recording calls with proper consent and HIPAA compliance, reviewing a statistically significant sample, and scoring those calls against your defined criteria. The goal is not surveillance. It is calibration. Your intake team needs to know what good looks like, and they need regular feedback to improve.
Build a review cadence that your operation can sustain. For centers handling 50-100 intake calls weekly, reviewing 10-15 calls per week provides enough data to identify patterns without overwhelming supervisors. Distribute reviews across intake team members, call types such as new inquiries, follow-ups, and insurance questions, and time periods, since morning calls often differ from evening calls.
The feedback mechanism is where most frameworks fail. Reviewing calls without delivering actionable feedback to the team is a waste of effort. Structure feedback sessions around specific, observable behaviors. Connect feedback to outcomes whenever possible.
Continuous improvement means your framework evolves. As your team improves on current benchmarks, raise the standard. As you identify new failure modes, add scoring criteria. As your center's clinical model changes, update what constitutes a successful call. This is not a static document. It is a living system that reflects your operation's growth.
The infrastructure required for a call quality framework includes call recording and storage compliant with HIPAA requirements for PHI, a scoring system ranging from a spreadsheet for smaller operations to dedicated QA software for larger ones, a review schedule with assigned responsibilities, and a feedback delivery process. Many treatment centers partner with paid media specialists who integrate call tracking with campaign attribution, creating a single view from ad click to call outcome.
Strategy
Ready to map a growth plan built for your vertical?
Scoring and Improving Intake Calls
Criteria that connect call performance to admissions outcomes
Intake call scoring translates qualitative call performance into quantifiable metrics. A well-designed scoring system identifies which behaviors correlate with successful admissions and which behaviors lose qualified callers. This is not about grading intake staff. It is about building a repeatable process that converts more inquiries into appropriate admissions.
Effective scoring criteria fall into several categories. Opening and rapport covers whether the intake specialist answered professionally, established a calm tone, and built initial trust. Needs assessment covers whether they asked appropriate questions to understand the caller's situation, treatment history, and immediate needs. Clinical alignment addresses whether they accurately represented your center's clinical model and determined fit. Logistics handling covers whether they addressed insurance, location, timing, and practical concerns efficiently. Call control covers whether they guided the conversation productively without rushing or losing the caller. Closing covers whether they established clear next steps and secured commitment where appropriate.
Weight your criteria based on what actually predicts admissions at your center. If your data shows that callers who complete insurance verification on the first call convert at twice the rate of those who do not, weight insurance handling heavily. If your data shows that calls over 12 minutes have diminishing returns, build talk time efficiency into your scoring. Let your outcomes drive your criteria.
The scoring scale matters less than consistency. Whether you use a 1-5 scale, a 1-10 scale, or a simple pass/fail on each criterion, the key is calibration across reviewers. Run regular calibration sessions where multiple reviewers score the same calls and discuss discrepancies. Without calibration, your scores measure reviewer preference, not call quality.
Use scores to identify training priorities. If your team consistently scores low on insurance verification, that is a training gap. If one team member scores high on rapport but low on closing, that is a coaching opportunity. Aggregate scores reveal systemic issues while individual scores reveal development needs. Both matter for intake process optimization.
Connect scoring to attribution data for the full picture. A call that scores 95% on your quality criteria but came from a low-intent keyword might still not convert. A call that scores 70% but came from a high-intent referral partner might convert despite the intake team's performance. Scoring tells you about your team. Attribution tells you about your leads. You need both to optimize the complete admissions funnel.
- Opening and rapport: Professional greeting, calm tone, trust-building language
- Needs assessment: Appropriate questions about situation, history, and immediate needs
- Clinical alignment: Accurate representation of treatment model and fit determination
- Insurance handling: Verification initiation, coverage explanation, financial discussion
- Call control: Productive guidance without rushing or losing caller engagement
- Closing strength: Clear next steps, commitment securing, follow-up scheduling
Connecting Call Quality with Admissions Success
Email Us
Prefer to talk it through over email?
The data that proves intake performance drives revenue
The connection between call quality and admissions success is not theoretical. It is measurable. Treatment centers that implement rigorous call quality frameworks and track outcomes consistently see higher conversion rates from inquiry to admission. The question is not whether the connection exists. The question is whether your operation has the infrastructure to see it.
Scaling through multi-market growth required building this infrastructure from scratch. Early in that growth, marketing generated leads and intake handled calls, but nobody could definitively say which marketing efforts produced admissions versus which produced inquiries that went nowhere. Implementing call quality scoring alongside admissions attribution tracking changed that. Within six months, the team could identify which referral sources produced callers who converted at 40%+ versus which sources produced callers who converted below 15%. That data drove reallocation decisions worth hundreds of thousands in annual marketing spend.
The pattern repeats across treatment centers of all sizes. A 45-bed residential program implemented call scoring and discovered that calls handled by their most experienced intake specialist converted at 38%, while calls handled by newer team members converted at 19%. The gap was not about effort or attitude. It was about specific, trainable behaviors: the experienced specialist asked about previous treatment attempts earlier in the call, addressed family involvement proactively, and moved to scheduling assessments more confidently. Training the full team on those specific behaviors closed the gap to 38% versus 31% within three months.
Attribution data amplifies these insights. When you know that calls from a specific Google Ads campaign convert at 28% while calls from a referral partner convert at 52%, and you also know that your call quality scores are consistent across both sources, you have isolated the variable. The lead source matters more than the intake performance for that comparison. Conversely, when two lead sources show similar conversion rates but dramatically different call quality scores, you have identified an intake issue masking a lead quality advantage.
The business case is straightforward. If your center handles 400 intake calls monthly and converts 25% to admissions, that is 100 admissions. If call quality improvements move that conversion rate to 30%, that is 120 admissions from the same lead volume. At an average revenue per admission of $15,000 to $30,000, depending on your model and payer mix, that improvement represents $300,000 to $600,000 in additional annual revenue. No additional marketing spend required.
Compliance and Regulatory Considerations
Building call quality systems that protect patients and your operation
Call quality management in behavioral health operates within strict regulatory boundaries. HIPAA governs how you handle protected health information on calls and in recordings. State regulations may impose additional requirements for consent, recording, and data retention. LegitScript certification, increasingly required for behavioral health marketing through major advertising platforms, includes standards for how treatment centers handle inquiries.
HIPAA compliance for call recording requires explicit consent from callers before recording begins. Many centers use automated disclosures followed by verbal confirmation. Recorded calls containing PHI must be stored securely, with access limited to authorized personnel. Retention periods should follow your organization's HIPAA policies and any applicable state requirements. The HHS Office for Civil Rights provides guidance on PHI handling that applies directly to call recording practices.
Call quality reviewers must be trained on PHI handling. Scoring sessions should focus on intake team performance, not on patient details. Documentation should reference call identifiers, not patient names. If your scoring system captures notes, those notes should address behaviors and techniques, not clinical information about callers.
LegitScript certification for treatment advertising includes standards around how facilities represent their services to prospective patients. Call quality frameworks should ensure that intake staff accurately describe your clinical model, avoid making outcome guarantees, and do not engage in patient brokering or other prohibited practices.
Google Ads and Meta both restrict advertising for addiction treatment services and prohibit retargeting in this vertical. Your attribution and call tracking systems must respect these restrictions. You cannot use call data to build retargeting audiences. You cannot track callers across the web after they contact your intake line. Your marketing approaches must operate within these boundaries while still delivering attribution insights.
Building compliance into your call quality framework from the start is easier than retrofitting it later. Document your consent processes. Train your team on PHI handling. Audit your recording storage regularly. Ensure your scoring criteria align with LegitScript standards for ethical intake practices. Compliance is not a constraint on quality improvement. It is a foundation that protects your patients and your operation.
Free Audit
Want a straight read on where your budget is leaking?
Building Your Intake Attribution Infrastructure
Practical steps to implement what this guide describes
Moving from concept to implementation requires a structured approach. Most treatment centers cannot build comprehensive intake attribution and call quality systems overnight. The goal is progressive improvement: start with foundational tracking, add call quality scoring, then connect the two into a unified feedback loop.
Phase one focuses on attribution fundamentals. Implement call tracking that captures source data for every intake call. Ensure your CRM records the inquiry source alongside caller information. Build a process for intake staff to confirm and update source data during calls. Establish baseline conversion metrics covering calls to assessments and assessments to admissions by source.
Phase two adds call quality infrastructure. Define your scoring criteria based on your clinical model and admissions process. Implement compliant call recording with proper consent. Train reviewers and calibrate scoring. Begin regular review cycles and feedback sessions. Track quality scores alongside conversion outcomes.
Phase three connects the systems. Analyze conversion rates by quality score. Identify which scoring criteria most strongly predict admissions. Adjust training priorities based on data. Report attribution and quality metrics together to identify whether conversion issues stem from lead quality or intake performance. Build this reporting into your regular operations review.
The investment is real but manageable. Call tracking typically costs $200-500 monthly, depending on volume. Call recording solutions range from basic options included in some phone systems to enterprise QA platforms at $500-2000 monthly. The larger investment is time: reviewing calls, providing feedback, and analyzing data requires dedicated effort. For centers managing $1.5M to $2M monthly in marketing spend, this investment pays for itself many times over through improved conversion rates and smarter budget allocation.
Treatment centers that want to accelerate this process often partner with agencies that specialize in behavioral health marketing and have existing infrastructure for attribution and call quality integration. Marketing Powered brings AI-native technology, tracked attribution through to admission, and operator-level experience across the behavioral health vertical.
Ready to Build Attribution and Call Quality Systems That Work?
Treatment centers with disciplined intake attribution and call quality frameworks convert more inquiries into admissions without increasing marketing spend. If your operation lacks visibility into which channels produce admissions or how your intake team performs against defined standards, that gap is costing you revenue. Marketing Powered brings AI-native technology, $50M+ in managed behavioral health media spend, and operator-level experience to help treatment centers build the infrastructure described in this guide. Let's discuss your current attribution setup, intake process, and where the opportunities are.
Questions, answered.
Intake attribution is the practice of tracking patient inquiries from their original marketing touchpoint through to admission. It connects specific marketing investments such as keywords, campaigns, and referral partners to actual admissions outcomes rather than just calls or form submissions. For treatment centers, this discipline reveals which channels produce qualified admissions versus which generate inquiries that do not convert, enabling smarter budget allocation and higher marketing ROI.
A call quality framework establishes standards for evaluating intake calls, implements monitoring through compliant call recording and review, and creates feedback loops for continuous improvement. Key components include defined scoring criteria matched to your clinical model, regular review cadences with calibrated reviewers, structured feedback sessions with intake staff, and benchmark tracking over time. The framework connects intake performance to admissions outcomes, identifying which specific behaviors correlate with conversion success.
Effective call scoring uses criteria that predict admissions outcomes at your specific center. Common categories include opening and rapport, needs assessment, clinical alignment, insurance handling, call control, and closing strength. Weight criteria based on your outcome data. Calibrate reviewers regularly to ensure consistency. Connect scores to attribution data to distinguish between intake performance issues and lead quality issues. Use aggregate scores to identify training priorities and individual scores to guide coaching.
Compliance protects both patients and your operation. HIPAA governs how you record, store, and access calls containing protected health information. LegitScript certification standards require ethical intake practices for treatment advertising eligibility. Google and Meta restrict behavioral health advertising and prohibit retargeting, which affects how you can use call data. Building compliance into your call quality framework from the start prevents costly retrofitting and protects your ability to market through major advertising platforms.
Ready to see what AI-native marketing can do for your treatment center?
Request a free audit of your paid media, landing pages, attribution, and compliance posture. You'll get a straight assessment of where the opportunities are.
or email us at info@marketingpowered.ai